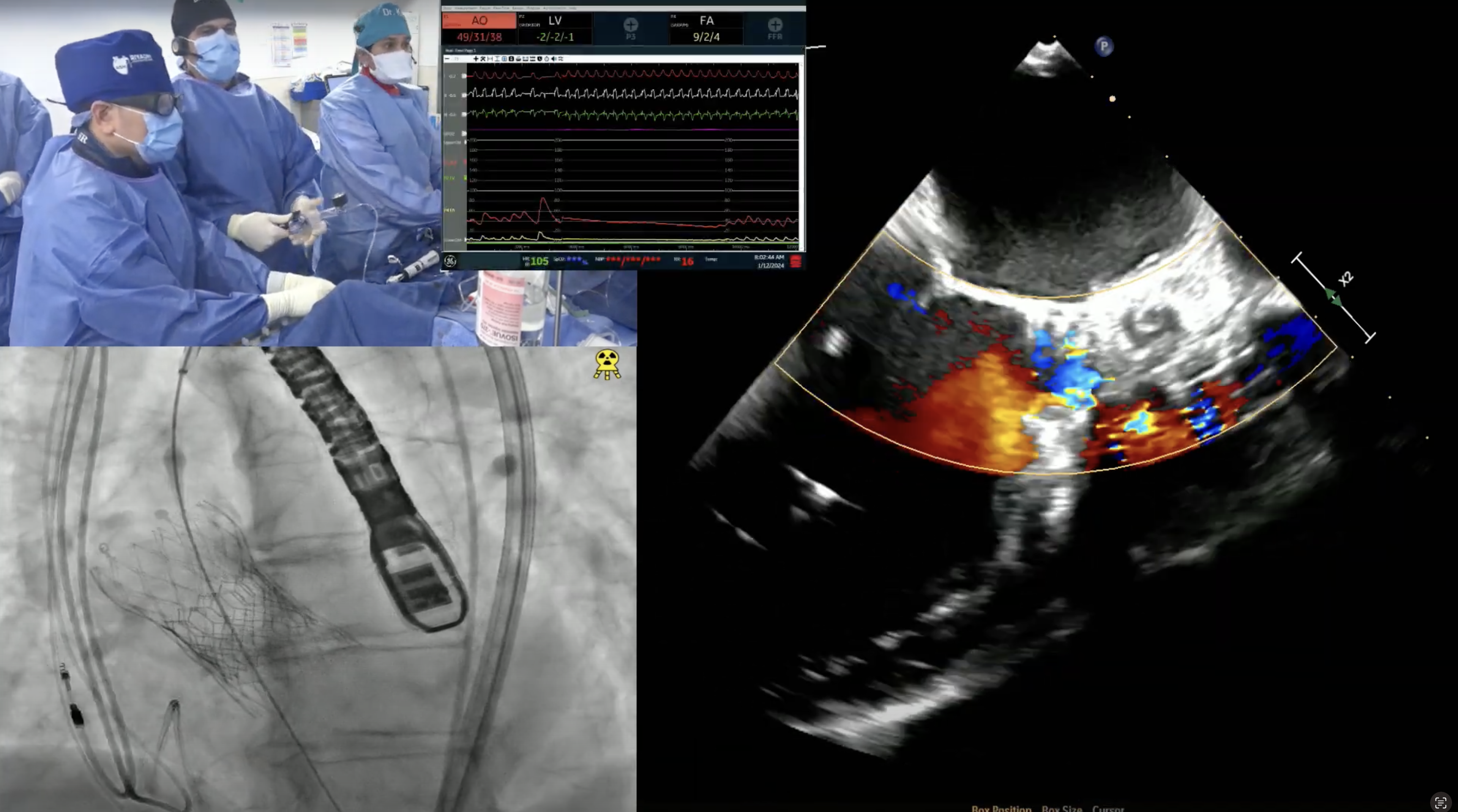
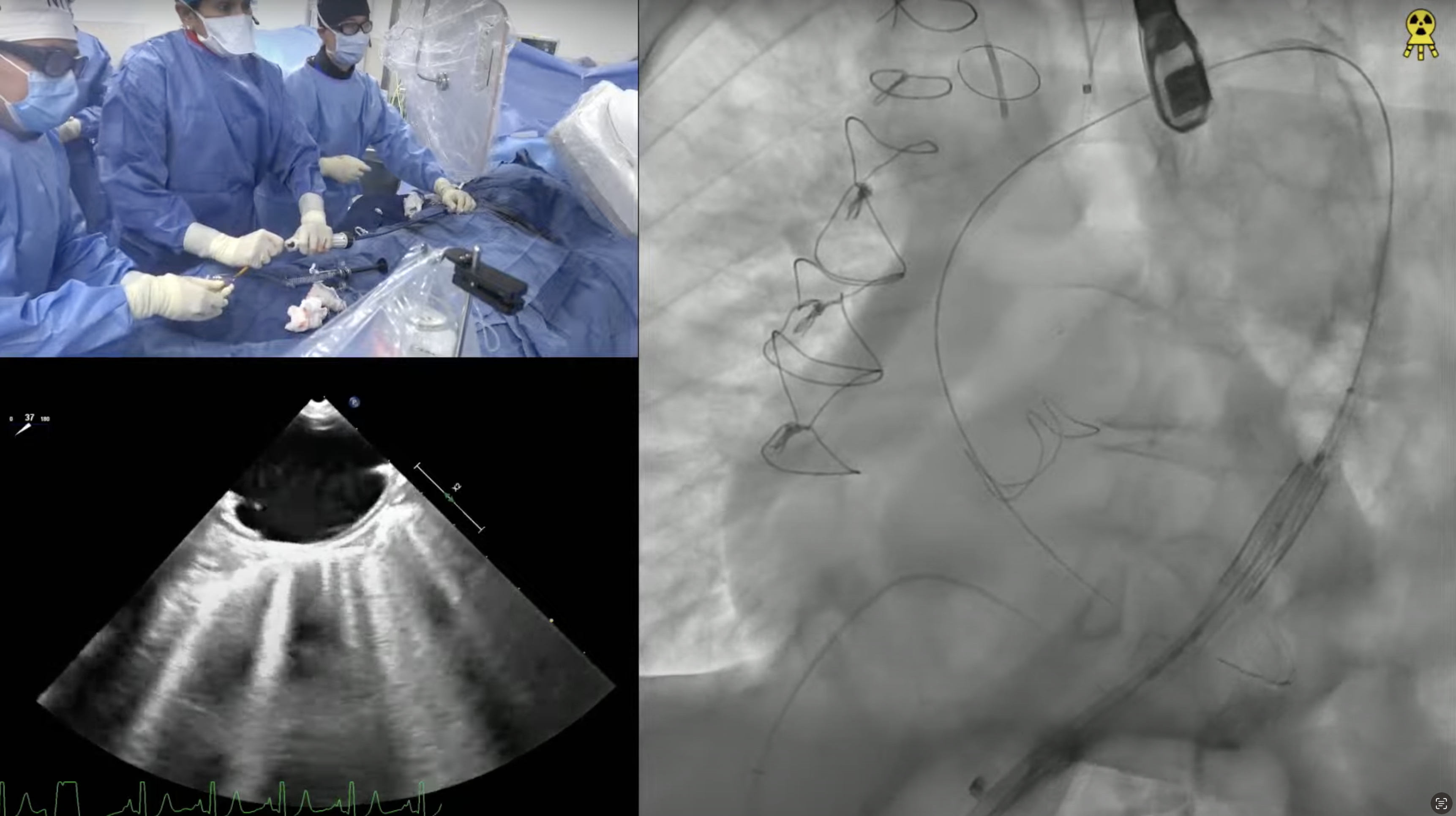
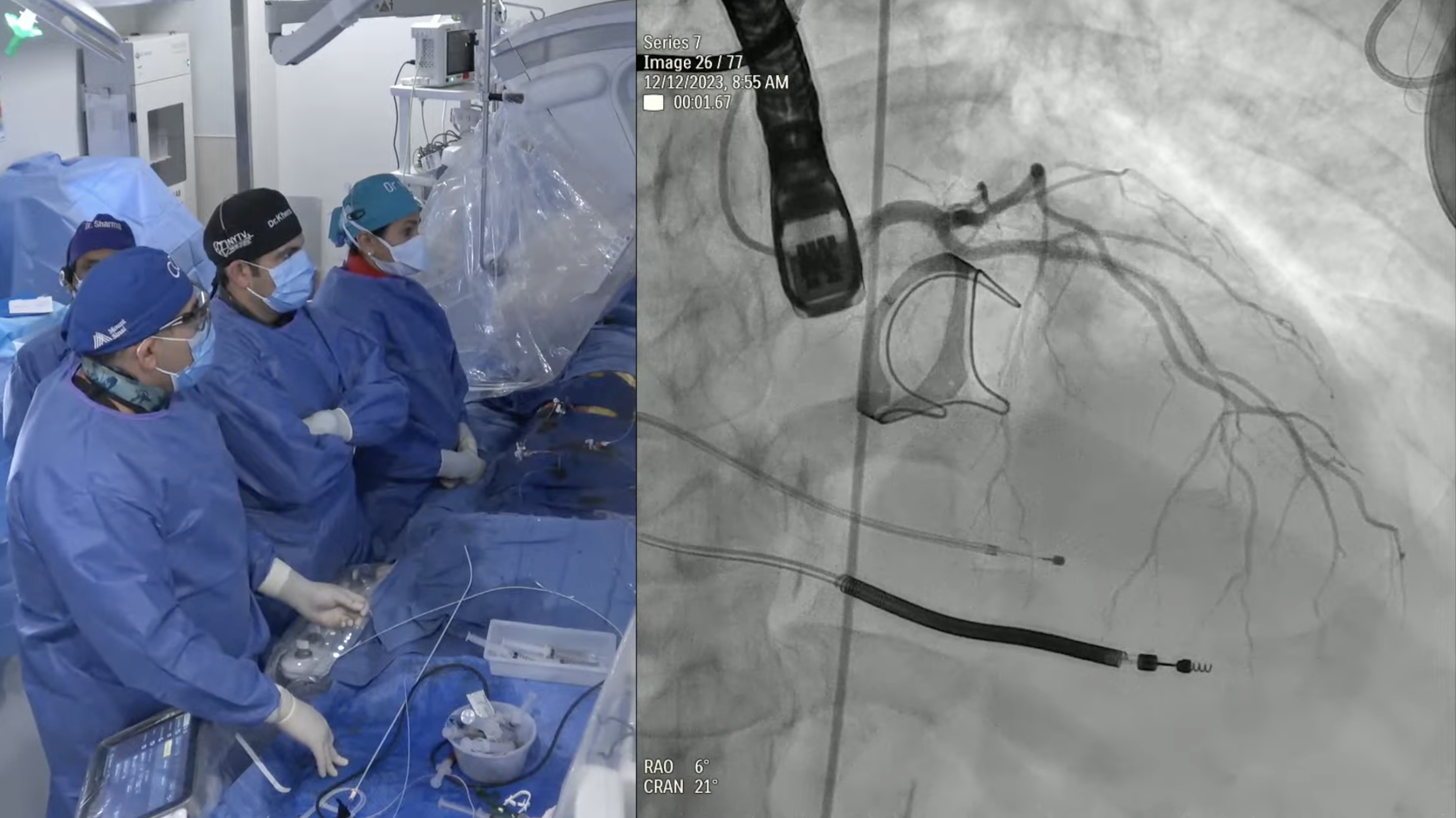
79 year old man presents with worsening exertional dyspnea (NYHA Class III) for the last 3 months. Patient has required multiple recent admissions to hospital with CHF exacerbation requiring IV diuretics. Past medical history is significant for symptomatic bicuspid aortic valve with dilated ascending aorta s/p Bentall procedure (2011) with 25 mm Carpentier-Edwards pericardial valve inside 30 mm Hemashield tube, atrial fibrillation on warfarin, hypertension, and dyslipidemia. Recent echocardiogram revealed bio-prosthetic valve degeneration with severe aortic regurgitation without significant stenosis and depressed LVEF of 40%. Coronary angiogram showed non-obstructive CAD. Analysis of lower extremities on CT angiogram revealed adequate diameters for trans-femoral approach. The Internal Diameter of surgical AV measured 22.1×25.7 mm (mean 23.9 mm), perimeter 76 mm and the area 454.8 mm2. The STS mortality risk for surgical AVR was 8.37% and logistic Euroscore mortality risk was 19.37%. The patient underwent Heart Team evaluation and was found to be at high risk for re-do SAVR due to comorbidities and frailty. Now presents for Valve-in-Valve TAVR with 26 mm SAPIEN-3 Valve +/- bio-prosthetic valve fracture via left percutaneous femoral approach with Sentinel cerebral protection device.