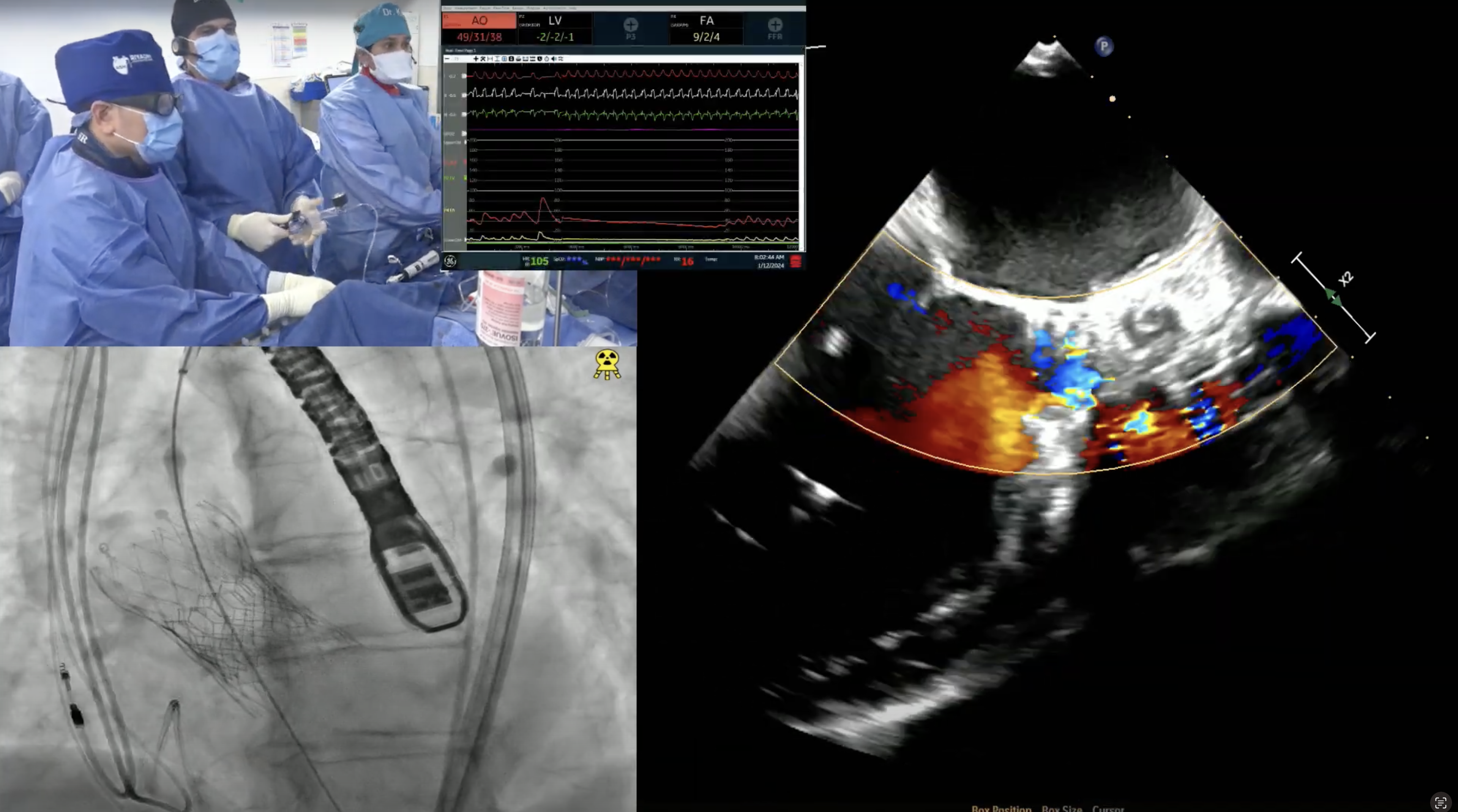
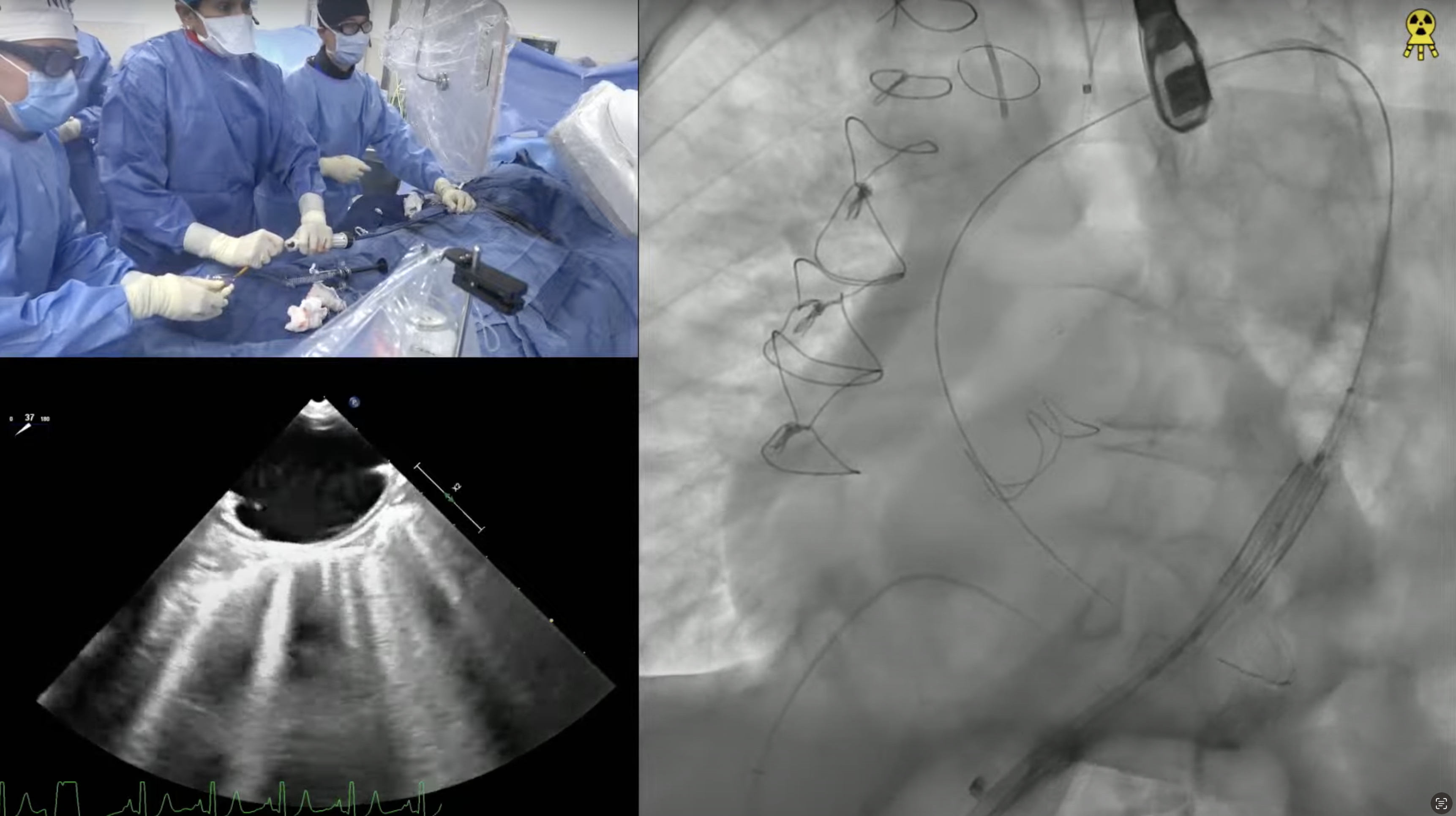
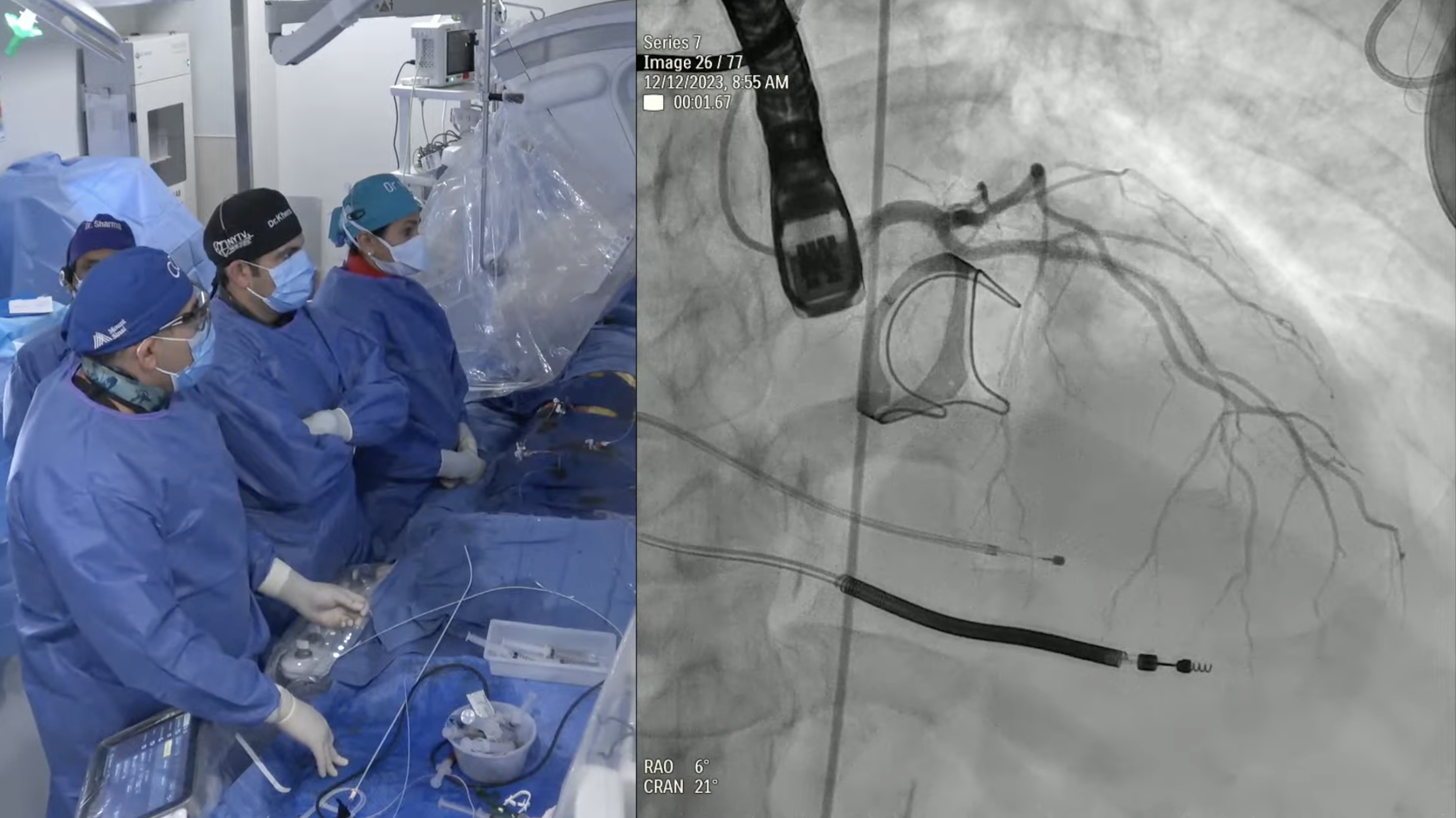
91 year old female presents with progressive exertional dyspnea (NYHA Class III) and decreased exercise tolerance <1 block for the last 2 months. Past medical history is significant for severe aortic stenosis s/p BAV on 11/21/16 (refused further therapy at that time), hypertension, hyperlipidemia, mild non-obstructive CAD, COPD, diverticulosis, osteoporosis and osteoarthritis. Recent echocardiogram revealed severe calcific aortic stenosis (PG/MG/AVA = 98mmHg/63mmHg/0.4cm2) and LVEF 64%. Analysis of lower extremity on CT angiogram revealed adequate diameter for trans-femoral approach. The aortic annulus measured 17.9 x 25.4 mm (mean 21.7 mm), annular perimeter was 70.5 mm and the annular area was 386.7 mm2. The STS mortality risk for surgical AVR was 9.19% and the logistic Euroscore mortality risk was 22.7%. The patient underwent Heart Team evaluation and was found to be at high risk for SAVR due to comorbidities, advanced age and frailty. Now presents for TAVR with 26 mm Evolut-PRO Corevalve via a right percutaneous femoral approach with Sentinel cerebral protection device.