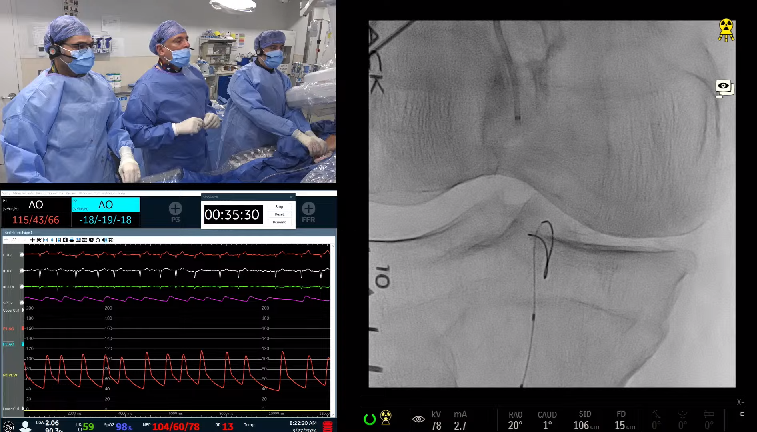
71 year old female with HTN, HLP, DM, complains of left LE claudication which progressed to resting pain (Rutherford 4). She underwent successful intervention of right SFA CTO using DES after failure of medical therapy. Initial peripheral angiogram showed ostial and long segment LSFA CTO with reconstitution in the distal segment.
great real world case where things don’t go perfect.
Appreciate love interaction. Poise under pressure.
As a vascular surgeon I would have managed the cfa issue surgically and via open groin performed the sfa intervention.